
Burnout vs Depression: How to Tell the Difference
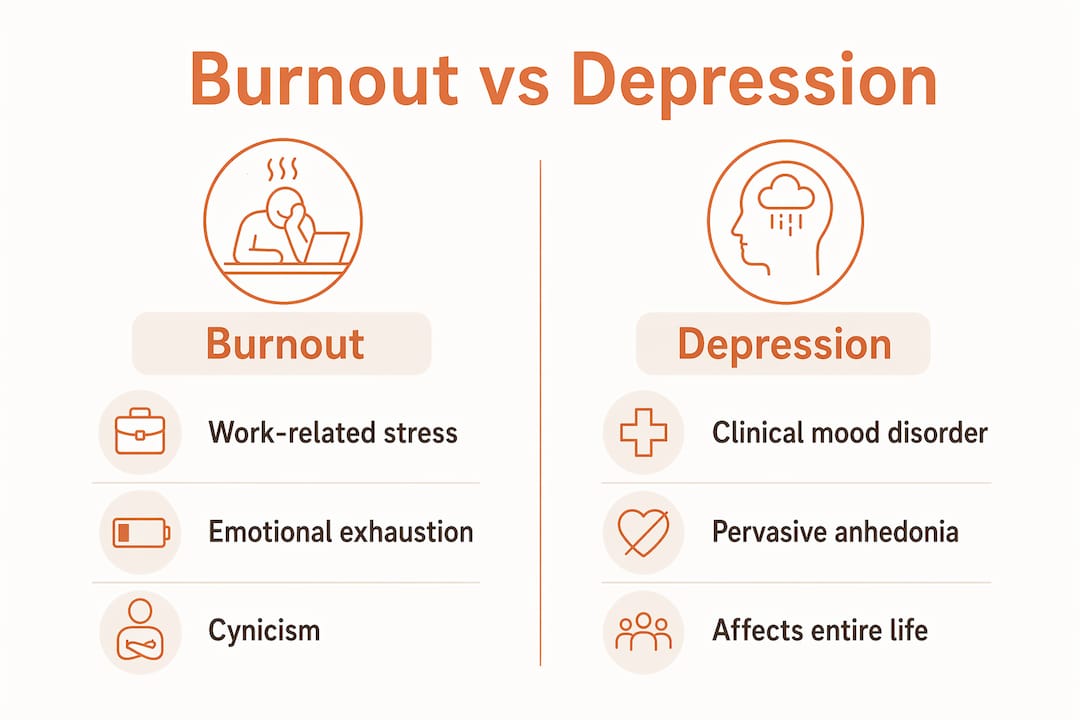
Burnout is defined as an occupational syndrome caused by chronic workplace stress, while depression is a clinical mood disorder that affects every area of life, not just work. Understanding the difference between burnout vs depression matters because the two conditions require different treatments. Choosing the wrong path delays recovery. If you feel exhausted, emotionally flat, or unable to function, knowing which condition you are dealing with is the first step toward feeling better.
What are the symptoms of burnout vs depression?
Burnout and depression share several symptoms, which is exactly why so many people confuse them. Both conditions produce fatigue and cognitive impairment, making it hard to concentrate, remember details, or stay motivated. The difference lies in where those symptoms show up and what drives them.
Burnout symptom profile
Burnout is characterized by three core features: emotional exhaustion, cynicism toward your work, and a reduced sense of personal accomplishment. You feel drained before the workday even starts. You may become detached, irritable with colleagues, or convinced that your efforts no longer matter. Critically, these feelings tend to ease when you step away from work, take a vacation, or change your environment.
Depression symptom profile
Depression causes pervasive anhedonia, meaning the loss of pleasure extends to hobbies, relationships, and activities that once brought joy. Physical symptoms appear too: changes in appetite, disrupted sleep, and psychomotor slowing, which is the feeling that your body and thoughts are moving through mud. Unlike burnout, depression symptoms persist across all settings regardless of rest or a change of scenery.

Side-by-side comparison
| Feature | Burnout | Depression |
|---|---|---|
| Primary cause | Chronic workplace stress | Multifactorial clinical disorder |
| Mood impact | Work-focused exhaustion | Pervasive low mood across all settings |
| Pleasure in hobbies | Usually preserved | Significantly reduced or absent |
| Physical symptoms | Fatigue, tension | Appetite changes, psychomotor slowing |
| Response to rest | Often improves | Persists despite breaks |
| Diagnostic framework | WHO occupational syndrome | DSM-5 major depressive disorder criteria |
Pro Tip: Track your mood over a weekend or during a vacation. If your energy and outlook improve significantly away from work, burnout is the more likely explanation. If low mood follows you everywhere, depression deserves serious consideration.
How do burnout and depression differ in causes and scope?
The clearest way to separate these two conditions is to look at scope of impact. Burnout is predominantly tied to workplace stress and leaves your capacity for joy outside of work largely intact. You can still laugh with friends on a Friday night, enjoy a meal, or feel engaged in a hobby. The problem is contained, even if it feels enormous.
Depression removes that boundary entirely. It affects your self-worth, your relationships, your physical health, and your ability to find meaning anywhere. The World Health Organization classifies burnout as an occupational syndrome, not a clinical disorder, while the DSM-5 classifies major depressive disorder as a condition requiring clinical treatment. That distinction shapes everything from diagnosis to recovery.
Self-identity is another key differentiator. Burnout patients typically feel they are failing at specific tasks or responsibilities. Depressed patients internalize that failure to their core sense of self, believing they are fundamentally broken or worthless as a person. This distinction in self-identity beliefs is one of the fastest clinical tools used to separate the two conditions.
Consider what happens when you imagine a perfect day off. A person with burnout can picture it clearly and feels genuine relief at the thought. A person with depression often cannot picture feeling better at all. That absence of hope is a signal worth taking seriously.
Can burnout lead to depression, and when should you seek help?
Burnout does not automatically become depression, but the risk is real and well-documented. Approximately 70% of individuals with severe burnout also meet the criteria for major depressive disorder. That overlap means untreated burnout is not just uncomfortable. It is a clinical risk factor.
The physiological toll of sustained burnout is significant. Chronic stress dysregulates cortisol, disrupts sleep architecture, and depletes the neurochemical reserves that support stable mood. Ignoring persistent burnout symptoms increases the likelihood that the condition will evolve into clinical depression, at which point rest alone is no longer sufficient.
Watch for these signs that burnout may have transitioned into depression:
- Low mood that persists on weekends, holidays, and during activities you used to enjoy
- Feelings of worthlessness or hopelessness that extend beyond your job
- Difficulty experiencing pleasure in any area of life, not just at work
- Thoughts of self-harm or that life is not worth living
- Physical symptoms like significant weight change or inability to sleep for weeks
Professional mental health evaluation is advised when low mood and exhaustion persist beyond situational stress. A licensed psychiatrist or psychologist can assess whether you meet the clinical criteria for depression and recommend the right treatment path. Waiting to see if it resolves on its own is the most common and costly mistake people make.
Pro Tip: After a full week away from work, note whether your energy starts to return. Restored energy after genuine rest points toward burnout. Continued flatness and hopelessness after rest points toward depression and warrants a clinical evaluation.
What practical strategies help you manage burnout or depression?
Recovery looks different depending on which condition you are dealing with. Getting the approach right matters more than acting fast.
Assessing your condition
The self-view test is a rapid clinical tool: ask yourself whether you feel like you are failing at your job, or whether you feel like a failure as a person. The self-view test differentiates burnout from depression by locating failure in job tasks versus personal identity. If failure feels task-specific, burnout is more likely. If failure feels like who you are, depression is more likely. You can also use a structured burnout or depression quiz from a licensed mental health resource to guide your self-assessment before seeking professional input.
Recovering from burnout
- Set firm work boundaries. Define your hours and protect them. Burnout thrives in environments without limits.
- Take genuine rest. A weekend of distraction is not recovery. Unstructured time, sleep, and physical activity rebuild depleted reserves.
- Change the environment when possible. Burnout is situational. Addressing the source, whether that means workload, management, or role fit, is part of recovery.
- Avoid self-medicating. Alcohol and stimulants mask burnout symptoms temporarily and accelerate the progression toward depression.
Treating depression
Depression requires clinical treatment. Therapy approaches like cognitive behavioral therapy, or CBT, directly address the distorted thinking patterns that sustain depression. Medication management, including antidepressants prescribed by a psychiatrist, corrects neurochemical imbalances that therapy alone cannot fix. Mindfulness practices and structured routines support treatment but do not replace it. Reviewing depression medication options with a qualified provider helps you understand what clinical intervention actually involves.
Pro Tip: Burnout patients who seek medication without changing their work environment often cycle back into burnout repeatedly. Medication treats symptoms, not the cause. Address the environment and the symptoms together for lasting recovery.
Key takeaways
Burnout is a work-specific syndrome that responds to rest and environmental change, while depression is a pervasive clinical disorder requiring professional treatment regardless of setting.
| Point | Details |
|---|---|
| Scope separates the two | Burnout stays at work; depression follows you everywhere, including into hobbies and relationships. |
| 70% overlap risk | Severe burnout meets clinical criteria for depression in most cases, making early intervention critical. |
| Self-view is a fast test | Feeling like you fail at tasks suggests burnout; feeling like you are a failure as a person suggests depression. |
| Rest reveals the answer | Energy that returns after genuine time off points to burnout; persistent flatness points to depression. |
| Treatment must match the condition | Burnout needs boundary-setting and environment change; depression needs therapy, medication, or both. |
Why getting the label right changes everything
People normalize chronic stress at a rate that genuinely concerns me. I have seen individuals spend months convinced they just need a vacation, only to return from two weeks off feeling exactly as hollow as when they left. That is not burnout. That is depression wearing burnout’s clothes.
The problem is that “burnout” has become a casual shorthand for any form of exhaustion. When the word loses clinical precision, people lose access to the right help. A person who is actually depressed may spend a year trying boundary-setting and rest, neither of which addresses the neurochemical and cognitive distortions driving their condition. That delay has real consequences for relationships, careers, and physical health.
What I find most useful is the self-identity question. When someone tells me they feel like a failure, I always ask: failure at what? If the answer is specific, “I can’t keep up with my caseload” or “I’m behind on every project,” burnout is on the table. If the answer is vague and total, “I’m just a failure,” that is a different conversation entirely. Recognizing the signs of depression early is not about labeling yourself. It is about getting the right support before the condition deepens.
Recovery from both conditions is real and achievable. The path just looks different depending on where you are starting from. Getting the diagnosis right is not a formality. It is the foundation of everything that follows.
— Jamie
Mental health support from Journeymhw
If you are unsure whether what you are experiencing is burnout or clinical depression, a professional evaluation removes the guesswork. Journeymhw offers online depression treatment for adults in Texas and Colorado, including psychiatric evaluations and medication management through a structured virtual care process. You do not need a referral or a long wait to get started.
Journeymhw’s licensed providers assess your symptoms, rule out overlapping conditions, and build a personalized treatment plan that fits your life. Whether you are managing the early signs of burnout or navigating a full depressive episode, professional support makes a measurable difference. Book an appointment and get clarity on what you are dealing with and what to do next.
FAQ
What is the main difference between burnout and depression?
Burnout is an occupational syndrome tied to chronic workplace stress, while depression is a clinical mood disorder that affects all areas of life. The key distinction is scope: burnout typically improves with rest and environment change, while depression persists regardless of setting.
Can burnout turn into depression?
Yes. Approximately 70% of individuals with severe burnout also meet the clinical criteria for major depressive disorder. Untreated burnout creates physiological and emotional conditions that increase the risk of developing clinical depression.
How do I know if I need professional help?
Seek a professional evaluation when low mood, exhaustion, or loss of pleasure persist beyond situational stress, especially if symptoms continue during time off work. A licensed psychiatrist can determine whether you meet the criteria for depression and recommend appropriate treatment.
Is there a burnout or depression quiz I can take?
Structured self-assessment tools exist, including validated scales like the Maslach Burnout Inventory for burnout and the PHQ-9 for depression. These are useful starting points, but a clinical evaluation from a licensed provider gives you the most accurate picture.
Does depression treatment differ from burnout recovery?
Burnout recovery centers on removing or reducing the workplace stressor, setting boundaries, and genuine rest. Depression treatment requires clinical intervention, typically cognitive behavioral therapy, medication management, or a combination of both, because the condition has neurochemical and cognitive components that lifestyle changes alone cannot resolve.